

- The doctor was unable to completely cut the tissue (the transverse carpal ligament) they intended.
- The surgery had to be terminated prematurely (usually due to respiratory or bleeding complications).
- Symptoms never resolved after the surgery.
Having a Second Carpal Tunnel Surgery?
From Dr. Z - Carpal tunnel syndrome specialist
Having a Second Carpal Tunnel Surgery?
Table of Contents
- When a second carpal tunnel surgery is recommended
- For doctors, carpal tunnel surgery failure means...
- For patients, carpal tunnel surgery failure means...
- The reality of what can happen after surgery
- Predicting the outcome of a second carpal tunnel surgery
- Dr. Beck's milestone "Outcome Predictor"
- Why have a second carpal tunnel surgery at all?
- Revision surgery is a gamble
- FAQs
- Summary
Many surgeons recommend their patients have a second carpal tunnel surgery after the first one failed. But it begs the question, “What’s the chance my second surgery will fail, too?” Statistically, your chances of a second carpal tunnel surgery failure are about 80%. That means a 20% success rate the second time around.
Therefore, it’s important for doctors to answer this question candidly: "Is a second carpal tunnel surgery really worth the risk?" After all, why suffer through another surgery when it might also fail?
- Suspect you have carpal tunnel? Complimentary self-test
- Already know you have carpal tunnel? Click here to learn its severity
When a second carpal tunnel surgery is recommended
Your first carpal tunnel release surgery has a statistical failure rate of 18-52%. This wide range depends on several factors. A primary factor is which medical journal reports the statistics.
The reporting of statistics heavily depends on how "surgical failure" is defined. Doctors and patients define failure differently.
For doctors, carpal tunnel surgery failure means...
For patients, carpal tunnel surgery failure means...

- By the second year, carpal tunnel symptoms returned.
- Complications (such as nerve damage, excessive bleeding, infection) were so great that the surgery wasn't worth the trouble.
- Significant Hand strength was permanently lost.
The reality of what can happen after surgery
However you define "surgical failure", the outcomes of carpal tunnel surgery fall into one of several categories.
- Complete failure from the outset.
The patient comes out of the operating room with no symptoms relief.
- Worsened symptoms.
The patient awakens from
anesthesia to find symptoms are worse than before surgery. This does not include
post-surgical pain, which is normal. Post-surgical pain generally disappears within 10 days from surgery.
- Return of symptoms. The patient has symptoms that return within days, weeks or months after the operation. Most hand surgeons consider it a surgical failure when carpal tunnel symptoms return within 6 months.
- Low satisfaction rate at 2 years. Perhaps the greatest contributor to surgical failure of carpal tunnel surgery is low patient satisfaction by the second year. The term "satisfaction" is highly subjective, but it's the real-world measure of whether or not patients are happy with their results. The published (and generally agreed upon) satisfaction rate for carpal tunnel surgery by year 2 is is 50%.
Predicting the outcome of a second carpal tunnel surgery
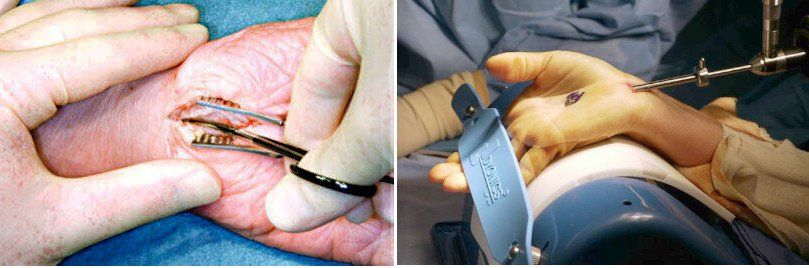
Often, a doctor will conclude you had a surgical failure if, for instance, your symptoms didn't resolve within 6 months. At that point, the doctor may recommend you have another surgery. This second carpal tunnel surgery is called "revision surgery".
Yes, that means having a second carpal tunnel surgery. That also means more pain, misery, expense, and loss of job time. Not to mention the extensive carpal tunnel recovery time and hand rehabilitation you'll need once again.
Many consciencious doctors began asking the obvious question, "If there is so much failure the first time, is there a way to predict the success of a second surgery?" Dr. John D. Beck (photo) studied this problem in detail.
In the journal American Society for Surgery of the Hand, Dr. Beck wrote a milestone article entitled Predicting the Outcome of Revision Carpal Tunnel Release. He studied patients over 2 years after they had a second carpal tunnel surgery. Some were successful the second time around. But some were failures once again.
For each patient, he looked back at their history within the previous 2 years. That helped him find correlations of past activities with the successes and failures he saw. Read about his "Outcome Predictor" below.
Dr. Beck's milestone "Outcome Predictor"
Dr. Beck quickly focused on a patient's prior steroid shots. He analyzed if the second surgery’s success could be predicted by the results of the prior injections. In other words...
If steroid shots had a positive effect on temporary pain relief, would shots also predict if a second carpal tunnel surgery would be successful?
His findings were clear. Over 80% of the time, if a patient obtained good temporary relief with steroid shots prior to surgery, then he/she would have relief after the second carpal tunnel surgery. If they didn’t get good steroid shot relief, then a second surgery would probably fail.
Therefore, prior steroid shot results are a good predictor of the second surgery’s outcome.
Dr. Beck said steroid shot results are a “good screening test” to establish future success with revision carpal tunnel surgery.

Why have a second carpal tunnel surgery at all?
The above discussion is startling in a very different way. Step back and ask yourself,
“What’s wrong with this logic?”
Let's say you had 1 or 2 steroid shots. Each time they worked fairly well until their effects wore off. Then your doctor recommended carpal tunnel surgery.
You had the first surgery -- but it failed. Then the doctor said, “Since the shots relieved symptoms at first, I recommend another carpal tunnel surgery because THIS TIME there's an 80% chance of success.”
That's NOT what Dr. Beck's findings suggest. Rather, published data shows revision surgery has a success rate of only 20%.

Revision surgery is a gamble
It's evident that a second carpal tunnel surgery is - at best - a gamble. But why are revision surgeries used at all?
Carpal tunnel surgery is pushed upon every patient by nearly every hand surgeon in America. I personally have several hand surgeon colleagues who do nothing but carpal tunnel surgery all week long. It's that lucrative.
So it’s no coincidence that carpal tunnel surgery is now the second most common surgical procedure. It's sort of a surgical epidemic.
As a result, general practitioners are now sounding the alarms. They recognize that many good, non-surgical carpal tunnel treatments are available right now. This is why many doctors are opting to recommend such treatments even before thinking about a first surgery - let alone a second carpal tunnel surgery.
Remedies like simple rest and avoidance, night bracing, hand and finger stretching exercises, and myofascial release massage are all effective for relieving carpal tunnel syndrome. And they don't require surgery.
For this reason, the American Academy of Orthopedic Surgeons (AAOS) published Clinical Guidelines on the Treatment of Carpal Tunnel Syndrome. In this doctor's guideline, the AAOS advises doctors to recommend ALL such non-surgical treatments FIRST, before even thinking about surgery.
Also, they recommend using non-surgical remedies even if the first surgery fails to resolve the symptoms within 7 weeks.

Summary
Are you considering having a second ("revision") carpal tunnel surgery because your first one failed? You can predict the success of your surgical outcome by how successful your prior steroid shots were. But does it really make sense to have another surgery if you didn't try all non-surgical options first?
FAQs
Is a second carpal tunnel surgery guaranteed to fail if the first one did?
No, but the success rate is only about 20%
Why does my surgeon recommend another surgery when I had one 4 years ago, but symptoms came back?
Some surgeons believe that the 20% success rate is a good gamble in patients with extreme pain or numbness.
How will I know if my first carpal tunnel surgery failed?
Symptoms will either be not resolved immediately after the operation, or else they will gradually return within 2-3 years.
About

Dr. Maik Zannakis (Dr. Z)
Medical Director at the CarpalRx
Dr. Z is an acclaimed medical scientist renowned for his expertise in carpal tunnel syndrome and soft tissue disorders. With over 40 years of experience, he is credited with hundreds of medical journal publications and hundreds more web articles about carpal tunnel syndrome. After inventing the CarpalRx, Dr. Z became the go-to expert for carpal tunnel syndrome and wrist tendonitis. His opinions, inventions, and personalized care have distinguished Dr. Z as a trusted leader in this growing field. Read full Bio
Click here to learn more about Dr. Z
Email: dr.z@carplarx.com
Phone: 800-450-6118